lv rv ratio|rv lv ratio pulmonary embolism : 2024-10-07 On echocardiogram, the IVC was more frequently not collapsible in patients with RV/LV ≥ 0.9 than those with a ratio 1:1 indicates RV dilation and should raise suspicion for elevated pulmonary pressures (Figure 2). Additionally, evaluating for septal flattening, or the ‘D’ sign, can be identified in the . De truien van adidas zijn verkrijgbaar in een verscheidenheid aan designs en kleuren, waardoor er altijd een stijlvolle optie is voor iedereen. Een van de populairste designs is .
0 · rv lv ratio radiopaedia
1 · rv lv ratio pulmonary embolism
2 · rv lv ratio on ct
3 · rv lv ratio normal
4 · rv lv ratio meaning
5 · rv lv ratio in pe
6 · rv lv ratio calculator
7 · how to measure rv lv ratio
8 · More
Alle Zwarte Adidas Yeezy sneakers Vergelijk alle aanbiedingen en SALE items uit mei Bekijk alle prijzen bij de verschillende winkels!Alle Adidas Yeezy sneakers maat 38 Vergelijk alle aanbiedingen en SALE items uit augustus Bekijk alle prijzen bij de verschillende winkels!
lv rv ratio*******This technology has been tested in randomized controlled trials using the endpoint of improvement in RV/left ventricular (LV) ratio because this predicts mortality and adverse outcomes. 17 Safety endpoints include major bleeding, mortality, and recurrent . The RV/LV ratio is determined by measuring the maximal RV and LV diameters from inner wall to inner wall on the axial slice that best approximates the four .
On echocardiogram, the IVC was more frequently not collapsible in patients with RV/LV ≥ 0.9 than those with a ratio <0.9. A small difference in overall IVC size was also .
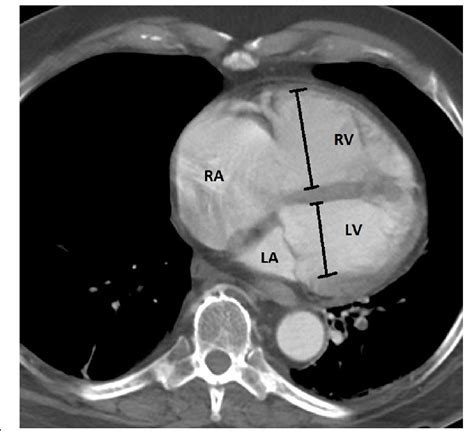
An RV:LV ratio >1:1 indicates RV dilation and should raise suspicion for elevated pulmonary pressures (Figure 2). Additionally, evaluating for septal flattening, or the ‘D’ sign, can be identified in the .Measurement of RV/LV ratio on CTPA is a clinically relevant skill to risk stratify patients with acute pulmonary embolism. We demonstrated that this skill was easily taught to .
Relative size of RV to LV should be assessed There is disproportionate enlargement of the . used to demonstrate RV dilatation. RV:LV ratio > 0.66 is abnormal* A thickened or .
The RV/LV diameter ratio, an established sign of RV dilatation on echo - cardiography, is among the most studied pa-rameters on pulmonary CTA [10–13]. One of the largest .
The kappa statistic for the presence of RV dilatation of the residents compared to the experienced radiologist ranged from 0.83–0.94. The average .The automated RV:LV ratio was compared with clinical reports to determine how this would have altered practice if it has been available at the time of the report. Results Entirely automated RV:LV analysis was .
The optimal cutoff value of RV/LV volume ratio to predict all-cause mortality was 2.32 (sensitivity = 87.5%; specificity = 87.0%) (Fig. 2a ). Thus, we defined “severe” .
Importantly, and in line with our earlier observations, RV/LV ratio >1.0 was present in 30% of patients treated at home . Overall, the number of adverse events in patients treated at home was low, independent of RV/LV ratio, and independent of the location of the PE, as was observed in the original Hestia and Vesta studies (6, 7).
TV E/A ratio, RV E′, post-bronchodilator FEV1/FVC, and use of oxygen during 6-minute walk test were independent predictors of exercise capacity. Pagourelias et al. (14) . Comparing the ratio of LV and RV basal dimensions in the 4-chamber view is a simple means of visually judging RV dilatation, but may not be valid if the LV itself is .On echocardiogram, the IVC was more frequently not collapsible in patients with RV/LV ≥ 0.9 than those with a ratio <0.9. A small difference in overall IVC size was also identified, with the RV/LV ≥ 0.9 group 0.2 cm larger, however this was not statistically significant. The left ventricular ejection fraction (LVEF) was no different between . This technology has been tested in randomized controlled trials using the endpoint of improvement in RV/left ventricular (LV) ratio because this predicts mortality and adverse outcomes. 17 Safety endpoints include major bleeding, mortality, and recurrent PE. Two primary approaches are currently used. The first, catheter-directed .All patients with PTE-related mortality had RV/LV ratio ≥1 in CTPA and had IVC reflux. Patients with an RV/LV ratio of ≥1 had statistically significantly higher troponin levels (p= 0.004) and IVC reflux (p= 0.025) compared to patients with an RV/LV ratio of <1. Conclusions: In conclusion, RV/LV ratio should be evaluated together with .rv lv ratio pulmonary embolismMeasurement of RV/LV ratio on CTPA is a clinically relevant skill to risk stratify patients with acute pulmonary embolism. We demonstrated that this skill was easily taught to trainees at all levels with simple instruction and was reproducible when viewing clinical images. Developing a teaching strategy for trainees at academic institutions to .
Considering all RV/LV ratio studies, the summary receiver operating characteristic (SROC) curve had an area under the curve (AUC) of 0.86 (0.83-0.89) for identifying the presence of RV dysfunction present on echocardiography. Overall, most studies were considered at high risk of bias. Subgroup analyses demonstrated that . An RV:LV ratio >1:1 indicates RV dilation and should raise suspicion for elevated pulmonary pressures (Figure 2). Additionally, evaluating for septal flattening, or the ‘D’ sign, can be identified in the parasternal short axis (PSS) mid-papillary view (Figure 3). Paradoxical septal motion can be visualized in both the PSS, subxiphoid, and . CTA is more widely accessible than echocardiography and is often the first imaging modality pursued in this clinical scenario. The most predictive indicator is the RV/LV ratio [13,16,17,18] as determined on transverse sections, and an RV/LV ratio ≥ 0.9 was linked to an elevated risk of clinical deterioration and mortality in prior studies .
The RV/LV ratio is determined by measuring the maximal RV and LV diameters from inner wall to inner wall on the axial slice that best approximates the four-chamber view (Fig. 9) . A value > 0.9 is considered abnormal.
A right ventricle/left ventricle (RV/LV) ratio >1.0 was not associated with fewer favorable outcomes in patients with symptomatic acute pulmonary embolism (PE) who were otherwise considered low risk, , according to study results published in The American Journal of Respiratory and Critical Care Medicine.. In this patient-level post . Submassive PE can also be diagnosed when RV enlargement on chest computed tomography, defined by an RV-to-LV diameter ratio >0.9, is observed. 18 RV enlargement on chest computed tomography predicts increased 30-day mortality in patients with acute PE. 18,19 Detection of RV enlargement by chest computed tomography is .The third E is for equality and this is really trying to estimate if the right ventricle is as big or bigger than the left ventricle. So normally the RV:LV ratio should be about 0.6 to 1 and this is classically measured in the apical four chamber view across the tips of the valves. We choose 1:1 as being abnormal because if you're getting the . The kappa statistic for the presence of RV dilatation of the residents compared to the experienced radiologist ranged from 0.83–0.94. The average interobserver difference in calculated RV/LV ratio’s (±SD) between the three residents was: -0.01 (SD0.11), 0.07 (SD0.14) and 0.06 (SD0.18) with an overall mean RV/LV diameter ratio .Several methods to determine RV dysfunction on computed tomographic pulmonary angiography (CTPA) have been proposed. According to the latest European Society of Cardiology (ESC) guideline, a right ventricle–to–left ventricle (LV) diameter ratio >1.0 is the most appropriate method for determining dysfunction ( 3, 4 ). the right ventricular outflow tract is considered enlarged when the measured diameter in the parasternal long axis exceeds 3.3 cm, or when the measured diameter exceeds 2.7 cm in the distal RVOT, as measured in the basal parasternal short axis view.
Volume management. Establish an adequate MAP. 2nd Tier: Often needed: Inhaled pulmonary vasodilators. Inotrope. 3rd Tier: Additional therapies. Intubation. Podcast. Questions & discussion. Pitfalls.lv rv ratio Volume management. Establish an adequate MAP. 2nd Tier: Often needed: Inhaled pulmonary vasodilators. Inotrope. 3rd Tier: Additional therapies. Intubation. Podcast. Questions & discussion. Pitfalls.
An increased RV:LV ratio measured at CTPA provides a simple, noninvasive method of risk stratification in patients with suspected ILD-PH. This should prompt closer follow-up, more aggressive treatment, and consideration of lung transplantation. Key Words. CT scan pulmonary. interstitial lung disease. pulmonary hypertension. right ventricle. The echocardiographically derived RV/LV endsystolic ratio (RV/LVes ratio) and the LV endsystolic eccentricity index (LVes EI), both measured in the parasternal short axis view, are potentially useful diagnostic variables for patients with suspected PH.lv rv ratio rv lv ratio pulmonary embolism Comparing the ratio of LV and RV basal dimensions in the 4-chamber view is a simple means of visually judging RV dilatation, but may not be valid if the LV itself is dilated. The most reproducible two-dimensional parameter for RV size is the RV basal diameter (RVD1), an important consideration when different sonographers perform serial . This technology has been tested in randomized controlled trials using the endpoint of improvement in RV/left ventricular (LV) ratio because this predicts mortality and adverse outcomes. 17 Safety endpoints include major bleeding, mortality, and recurrent PE. Two primary approaches are currently used. The right ventricle (RV) is constructed to accommodate a low-resistance afterload. Increases in afterload from acute massive and submassive PE and CTEPH may markedly compromise the RV function leading to hemodynamic collapse and death.
Specificaties: Pasvorm: regular fit jack en slim-fit broek/ elastische tailleband met aantrekkoord in de broek. Manchetten: elastische manchetten aan de .
lv rv ratio|rv lv ratio pulmonary embolism